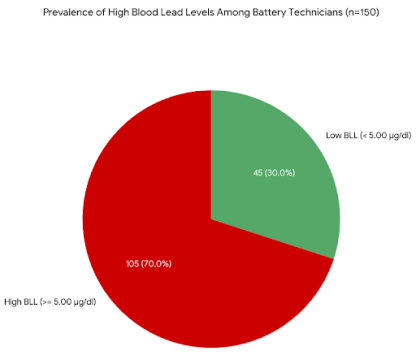
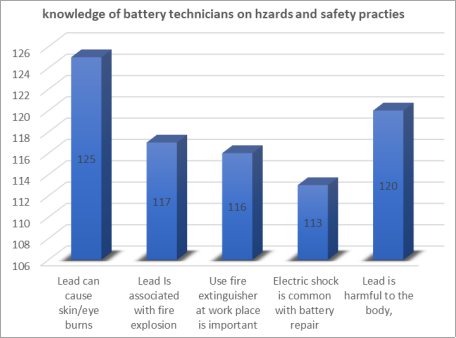
Battery technicians who repair lead-acid batteries are consistently exposed to elemental lead, which poses a significant occupational health risk. This exposure is associated with an elevated risk of developing serious lead related diseases and long-term disability. Understanding the interplay between occupational practices, knowledge of hazards, and actual lead exposure is critical for developing effective public health interventions in this high-risk occupational group. The primary objective of this study was to comprehensively assess the blood lead levels (BLLs) of battery technicians, and evaluate their current knowledge of lead health hazards, their attitude towards preventive measures, their adherence to safety practices, and their general work habits. This investigation employed a descriptive cross-sectional study design. The study population comprised a total of 150 currently active battery technicians operating within a defined geographical area. Data collection was performed using a structured, pre-tested, self-administered questionnaire. This instrument gathered information on socio-demographics, detailed knowledge of lead's health hazards, specific safety practices utilized, and daily work and personal hygiene habits. The BLLs were concurrently measured for all participants using an appropriate laboratory technique. Statistical analysis, including the Chi-square test, was performed using the Statistical Package for Social Sciences (SPSS), version 20, to test for significant associations, with the significance level set at p≤0.05. Analysis of the data revealed that a substantial proportion of the technicians exhibited elevated BLLs. Key findings indicated that knowledge regarding the appropriate use of a rubber apron, attitude towards the inhalation of lead fumes, and the crucial habit of face washing before eating/smoking were all significantly associated with the measured blood lead level of the battery technicians (p≤0.05). These results underscore that specific behavioral practices directly correlate with the biological burden of lead exposure. The study concludes that there is an urgent need to improve occupational hygiene and health literacy among battery technicians. It is strongly recommended that workplaces ensure the provision and mandatory use of personal protective equipment (PPE), particularly rubber aprons and face masks. Furthermore, intensified health education and regular training on the proper use of PPE, the provision of readily available running water at all workplaces for personal hygiene, and targeted behavioral change communication are essential strategies that will promote consistent personal hygiene habits and, ultimately, reduce the significant occupational lead burden for this vulnerable workforce.
| Published in | Science Journal of Public Health (Volume 13, Issue 6) |
| DOI | 10.11648/j.sjph.20251306.13 |
| Page(s) | 338-347 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Health Hazards, Safety Practices, Work Habits
Variables | Battery technicians (n=150) |
|---|---|
Age group (years) | |
21-30 | 17 (11.3) |
31-40 | 47 (31.3) |
41-50 | 49 (32.7) |
51-60 | 20 (13.3) |
>60 | 17 (11.3) |
Level of education | |
No formal education | 8 (5.3) |
Primary | 72 (48.0) |
Secondary | 63 (42.0) |
Tertiary | 7 (4.7) |
Years of work | |
0-9 | 29 (19.3) |
10-19 | 49 (32.7) |
20 and above | 72 (48.0) |
Daily work hours | |
0 -8 | 43 (28.7) |
>8 | 107 (71.3) |
Had training on first aid | 52 (34.7) |
Attitude regarding hazards and safety practices | Strongly agree (%) | Agree | Not sure | Disagree | Strongly disagree |
|---|---|---|---|---|---|
Hand washing prevents lead poisoning | 2 (1.3) | 6 (4.0) | 3 (2.0) | 58 (38.7) | 81 (54.0) |
Gloves protect against electric shock | 6 (4.0) | 11 (7.3) | 4 (2.7) | 44 (29.3) | 85 (56.7) |
Breathing in lead fumes is harmful | 5 (3.3) | 6 (4.0) | 8 (5.3) | 36 (24.0) | 95 (63.3) |
Face shield is important during repair | 12 (8.0) | 17 (11.3) | 10 (6.7) | 46 (30.7) | 65 (43.3) |
Smoking at workplace is harmful | 12 (8.0) | 19 (12.7) | 12 (8.0) | 29 (19.3) | 78 (52.0) |
Eating at workplace is harmful | 18 (12.0) | 33 (22.0) | 8 (5.3) | 31 (20.7) | 60 (40.0) |
Overall positive attitude score = 76 (50.7%) |
Variables | Possession n=150 | Usage n=150 | |||
|---|---|---|---|---|---|
Always (%) | Sometimes (%) | Never (%) | |||
Personal protective equipment | |||||
Eye goggles | 45 (30.0) | 29 (19.3) | 16 (10.7) | 105 (70.0) | |
Face shield | 36 (24.0) | 23 (15.3) | 13 (8.7) | 114 (76.0) | |
Rubber apron | 75 (50.0) | 51 (34.0) | 24 (16.0) | 75 (50.0) | |
Rubber gloves | 73 (48.7) | 50 (33.3) | 27 (18.0) | 73 (48.7) | |
Workplace habits | |||||
Wash hands before eating | 137 (91.3) | 12 (8.0) | 1 (0.7) | ||
Wash face before eating | 61 (40.7) | 31 (20.7) | 58 (19.7) | ||
Bathe after work | 115 (76.7) | 27 (18.0) | 8 (5.3) | ||
Change clothes before going home | 136 (90.7) | 8 (5.3) | 6 (4.0) | ||
Live/sleep at workplace | 22 (14.7) | 38 (25.3) | 90 (60.0) | ||
Overall practice score = 69 (46%) | |||||
Variables | BLL (µg/dl) n=150 | χ2 | df | p | |
|---|---|---|---|---|---|
<5.00 | ≥5.00 | ||||
Age group (years) | |||||
<40 | 15 (27.3) | 40 (72.7) | |||
40-59 | 19 (24.7) | 58 (75.3) | 9.53 | 2 | 0.009* |
≥60 | 11 (61.1) | 7 (38.9) | |||
Education | |||||
No formal education | 3 (37.5) | 5 (62.5) | |||
At least primary | 42 (29.6) | 100 (70.4) | 0.23 | 1 | 0.697 |
Years of work | |||||
0-9 | 6 (20.7) | 23 (79.3) | |||
≥10 | 39 (32.2) | 82 (67.8) | 1.48 | 1 | 0.223 |
Daily work hours | |||||
0 -8 | 13 (30.2) | 30 (69.8) | |||
>8 | 32 (29.9) | 75 (70.1) | 0.02 | 1 | 0.969 |
Variables | BLL (µg/dl) n=150 | χ2 | df | P value | |
|---|---|---|---|---|---|
<5.00 | ≥5.00 | ||||
Cause skin/eye burns | |||||
Yes | 38 (30.4) | 87 (69.6) | |||
No | 7 (28.0 | 18 (72.0) | 0.06 | 1 | 0.811 |
Cause fire explosion | |||||
Yes | 34 (29.1) | 83 (70.9) | |||
No | 11 (33.3) | 22 (66.7) | 0.22 | 1 | 0.636 |
Requires possession of fire extinguishers | |||||
Yes | 31 (27.0) | 84 (73.0) | |||
No | 14 (41.2) | 20 (58.8) | 2.52 | 1 | 0.113 |
Associated with electric shock | |||||
Yes | 35 (31.0) | 78 (69.0) | |||
No | 10 (27.0) | 27 (73.0) | 0.21 | 1 | 0.649 |
Battery lead is harmful to the body | |||||
Yes | 37 (30.8) | 83 (69.2) | |||
No | 8 (26.7) | 22 (73.3) | 0.20 | 1 | 0.656 |
Requires use of rubber aprons | |||||
Yes | 35 (26.5) | 95 (73.1) | |||
No | 10 (50.0) | 10 (50.0) | 4.40 | 1 | 0.036* |
Handwashing prevents lead poisoning | |||||
Strongly agree/agree | 42 (30.2) | 97 (69.8) | |||
Not sure | 1 (33.3) | 2 (66.7) | 0.34 | 2 | 1.000 |
Strongly disagree/disagree | 2 (25.0) | 6 (75.0) | |||
Gloves protect against electric shock | |||||
Strongly agree/agree | 40 (31.0) | 89 (69.0) | |||
Not sure | 1 (25.0) | 3 (75.0) | 0.44 | 2 | 0.908 |
Strongly disagree/disagree | 4 (23.5) | 13 (76.5) | |||
Inhaling lead fumes is harmful | |||||
Strongly agree/agree | 35 (21.0) | 93 (79.0) | |||
Not sure | 6 (75.0) | 2 (25.0) | 8.97 | 2 | 0.009* |
Strongly disagree/disagree | 1 (9.1) | 10 (90.9) | |||
Face shields are necessary while working | |||||
Strongly agree/agree | 31 (27.9) | 80 (72.1) | |||
Not sure | 4 (40.0) | 6 (60.0) | 0.98 | 2 | 0.612 |
Strongly disagree/disagree | 10 (34.5) | 19 (65.5) | |||
Smoking at workplace is harmful | |||||
Strongly agree/agree | 34 (31.8) | 73 (68.2) | |||
Not sure | 2 (16.7) | 10 (83.3) | 1.19 | 2 | 0.551 |
Strongly disagree/disagree | 9 (29.0) | 22 (71.0) | |||
Eating at workplace is harmful | |||||
Strongly agree/agree | 27 (29.7) | 64 (70.3) | |||
Not sure | 4 (50.0) | 4 (50.0) | 1.69 | 2 | 0.430 |
Strongly disagree/disagree | 14 (27.5) | 37 (72.5) | |||
Wash hands before eating | |||||
Always | 44 (32.1) | 93 (67.9) | |||
Sometimes | 1 (8.3) | 11 (91.7) | 3.285 | 2 | 0.130 |
Never | 0 (0.0) | 1 (100.0) | |||
Wash face before eating | |||||
Always | 25 (41.7) | 35 (58.3) | |||
Sometimes | 22 (71.0) | 9 (29.0) | 7.53 | 2 | 0.023* |
Never | 11 (18.6) | 48 (81.4) | |||
Bathe after work | |||||
Always | 37 (32.2) | 78 (67.8) | |||
Sometimes | 6 (22.2) | 21 (77.8) | 1.13 | 2 | 0.568 |
Never | 3 (25.0) | 6 (75.0) | |||
Change clothes before going home | |||||
Always | 39 (28.7) | 97 (71.3) | |||
Sometimes | 3 (37.5) | 5 (62.5) | 1.47 | 2 | 0.479 |
Never | 3 (50.0) | 3 (50.0) | |||
Live/sleep at workplace | |||||
Always | 9 (40.9) | 13 (59.1) | |||
Sometimes | 9 (23.7) | 29 (76.3) | 1.969 | 2 | 0.374 |
Never | 27 (30.0) | 63 (70.0) | |||
BLLs | Blood Lead Levels |
EDTA | Ethylenediaminetetraacetic Acid |
HREC | Health Research Ethics Committee |
PPE | Personal Protective Equipment |
SPSS | Statistical Package for Social Sciences |
| [1] | Peter AO. Total blood and urinary lead levels in battery charging artisans in two metropolitan cities of South West Nigeria. Nigerian Journal of Physiological Sciences. 2009; 14: 796-9. |
| [2] | Haider MJ, Qureshi N. Studies on battery repair and recycling workers occupationally exposed to lead in Karachi. Journal of Pakistan Medical Association. 2013; 64(1): 37-42. |
| [3] |
Adela Y, Ambelu A, Tessema DA. Occupational lead exposure among automotive garage workers - a case study for Jimma town, Ethiopia. Journal of Occupational Medicine and Toxicology. 2012; 7: 15. HYPERLINK "
https://doi.org/" https://doi.org/10.1186/1745-6673-7-15 |
| [4] | Fewtrell L, Kaufmann R, Prüss-Üstün A. Assessing the environmental burden of disease at national and local levels. Environmental Burden of Disease Series. 2003; n 2. |
| [5] | Tong S, von Schirnding YE, Prapamontol T. Environmental lead exposure: a public health problem of global dimensions. Bull World Health Organ. 2000; 78(9): 1068-77. |
| [6] |
Chuang HY, Lee ML, Chao KY, Wang JD, Hu H. Relationship of blood lead levels to personal hygiene habits in lead battery workers: Taiwan, 1991-1997. Am J Ind Med. 1999; 35(6): 595-603. HYPERLINK "
https://doi.org/" https://doi.org/10.1002/(sici)1097-0274(199906)35:6<595::aid-ajim10>3.0.co;2-8 |
| [7] |
Askin DP, Volkmann M. Effect of personal hygiene on blood lead levels of workers at a lead processing facility. Am Ind Hyg Assoc J. 1997; 58(10): 752-3.
HYPERLINK "
https://doi.org/" https://doi.org/10.1080/15428119791012971 |
| [8] |
Karita K, Shinozaki T, Tomita K, Yano E. Possible oral lead intake via contaminated facial skin. Science of the Total Environment. 1997 Jun 20; 199(1-2): 125-31.
HYPERLINK "
https://doi.org/" https://doi.org/10.1016/s0048-9697(97)00072-6 |
| [9] | Johnson OE, Bassey EA. Work Habits and Health Problems of Automobile Technicians at Mechanic Village, Uyo, Nigeria. Glob Adv Res J Med Med Sci. 2016; 5(5): 136-42. |
| [10] |
Ozomata EA, Odugbemi TO, Osagiede EF. A Study of Knowledge of Occupational Health Hazards and Safety Practices among Automobile Mechanics in an Urban Area of South-Western Nigeria. Nigerian medical journal. 2021; 62: 104-12. HYPERLINK "
https://doi.org/" https://doi.org/10.4103/nmj.nmj_190_20 |
| [11] |
Awodele O, Popoola TD, Ogbudu BS, Akinyede A, Coker HAB, Akintonwa A. Occupational hazards and safety measures amongst the paint factory workers in Lagos, Nigeria. Saf Health Work. 2014; 5(2): 106-11.
HYPERLINK "
https://doi.org/" https://doi.org/10.1016/j.shaw.2014.02.001 |
| [12] | Prabhakar GN. Sample size determination. Textbook of Biostatistics. Jaypee Brothers Medical Publishers Ltd; 2006. p. 110-19. |
| [13] | Elder S. School to work transition survey: A methodological guide. International Labour Office, Geneva. 2009. p. 1-40. |
| [14] | Olugbenga-bello Adenike I, Esther A Olarinmoye, Adefisoye A, Adeleye A, Sunday O. Perception, attitude and involvement of men in maternal health care in a Nigerian community. J Public Heal Epidemiol. 2013; 5(6): 262-70. |
| [15] | CDC. Blood Lead Level Guidance. 2024; |
| [16] |
Malekirad AA, Kalantari-Dehaghi R, Abdollahi M. Clinical, haematological, and neurocognitive findings in lead-exposed workers of a battery plant in Iran. Arh Hig Rada Toksikol. 2013; 64(4): 497-503.
HYPERLINK "
https://doi.org/" https://doi.org/10.2478/10004-1254-64-2013-2415 |
| [17] |
Fenga C, Cacciola A, Martino LB, Calderaro SR, Di Nola C, Verzera A, et al. Relationship of blood lead levels to blood pressure in exhaust battery storage workers. Ind Health. 2006; 44(2): 304-9. HYPERLINK "
https://doi.org/" https://doi.org/10.2486/indhealth.44.304 |
| [18] | Kianoush S, Balali-Mood M, Mousavi SR, Shakeri MT, Dadpour B, Moradi V, et al. Clinical, toxicological, biochemical, and hematologic parameters in lead exposed workers of a car battery industry. Iran J Med Sci. 2013; 38(1): 30-7. |
| [19] | Keramati MR, Sadeghian MH, Mood M. Correlation Between Iron Deficiency and Lead Intoxication in the Workers of a Car Battery Plant. Int J Hematol Oncol. 2010; 20(3): 169-75. |
| [20] |
Ahmad SA, Khan MH, Khandker S, Sarwar a FM, Yasmin N, Faruquee MH, et al. Blood lead levels and health problems of lead Acid battery workers in Bangladesh. ScientificWorldJournal. 2014; 2014: 1-5.
HYPERLINK "
https://doi.org/" https://doi.org/10.1155/2014/394628 |
| [21] |
Alasia DD, Emem-Chioma PC WF. Association of Lead Exposure, Serum Uric Acid and Parameters of Renal Function in Nigerian Lead- Exposed Workers. Int J Occup Environ Med. 2010; 1(4): 182-90.
HYPERLINK "
https://doi.org/" https://doi.org/10.15171/ijoem.2010.1.4.182 |
| [22] | Saliu A, Adebayo O, Kofoworola O. Comparative Assessment of Blood Lead Levels of Automobile Technicians in Organised and Roadside Garages in Lagos, Nigeria. 2015. |
| [23] | Mwatu AK. Health hazards associated with spray painting among workers in small scale auto garages in Emabakasi division, Nairobi, Kenya. Master's Thesis. 2011. |
| [24] | Monney I, DwumfourAsare B, OwusuMensah I, Kuffour R. Occupational health and safety practices among vehicle repair artisans in an urban area in Ghana. J Environ Occup Sci. 2014; 3(3): 1. |
| [25] |
Ajayi IA, Adeoye AO, Bekibele CO, Onakpoya OH, Omotoye OJ. Awareness and utilization of protective eye device among welders in a southwestern Nigeria community. Ann Afr Med. 2011; 10(4): 294-9. HYPERLINK "
https://doi.org/" https://doi.org/10.4103/1596-3519.85664 |
| [26] | Nasab H, Tavakoli R, Ghofranipour F. Evaluation of Knowledge, Attitude and Behavior of Workers towards Occupational Health and Safety. Iran J Public Health. 2009; 38(2): 125-9. |
| [27] |
Yu ITS, Lee NL, Wong TW. Knowledge, attitude and practice regarding organic solvents among printing workers in Hong Kong. J Occup Health. 2005; 47(4): 305-10.
HYPERLINK "
https://doi.org/" https://doi.org/10.2486/indhealth.47.305 |
| [28] |
Kim KR, Lee SW, Paik NW, Choi K. Low-level lead exposure among South Korean lead workers, and estimates of associated risk of cardiovascular diseases. J Occup Environ Hyg. 2008; 5(6): 399-416. HYPERLINK "
https://doi.org/" https://doi.org/10.1080/15298660802102195 |
APA Style
Ozomata, E. A., Maduafokwa, B. A., Giwa, O., Igwilo, U. A., Osagiede, E. F. (2025). Assessment of Blood Lead Level and Knowledge of Health Hazards, Safety Practices and Work Habits Amongst Battery Technicians in Nigeria. Science Journal of Public Health, 13(6), 338-347. https://doi.org/10.11648/j.sjph.20251306.13
ACS Style
Ozomata, E. A.; Maduafokwa, B. A.; Giwa, O.; Igwilo, U. A.; Osagiede, E. F. Assessment of Blood Lead Level and Knowledge of Health Hazards, Safety Practices and Work Habits Amongst Battery Technicians in Nigeria. Sci. J. Public Health 2025, 13(6), 338-347. doi: 10.11648/j.sjph.20251306.13
AMA Style
Ozomata EA, Maduafokwa BA, Giwa O, Igwilo UA, Osagiede EF. Assessment of Blood Lead Level and Knowledge of Health Hazards, Safety Practices and Work Habits Amongst Battery Technicians in Nigeria. Sci J Public Health. 2025;13(6):338-347. doi: 10.11648/j.sjph.20251306.13
@article{10.11648/j.sjph.20251306.13,
author = {Ebenezer Adeiza Ozomata and Blossom Adaeze Maduafokwa and Opeyemi Giwa and Uzoamaka Allena Igwilo and Emmanuel Friday Osagiede},
title = {Assessment of Blood Lead Level and Knowledge of Health Hazards, Safety Practices and Work Habits Amongst Battery Technicians in Nigeria},
journal = {Science Journal of Public Health},
volume = {13},
number = {6},
pages = {338-347},
doi = {10.11648/j.sjph.20251306.13},
url = {https://doi.org/10.11648/j.sjph.20251306.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251306.13},
abstract = {Battery technicians who repair lead-acid batteries are consistently exposed to elemental lead, which poses a significant occupational health risk. This exposure is associated with an elevated risk of developing serious lead related diseases and long-term disability. Understanding the interplay between occupational practices, knowledge of hazards, and actual lead exposure is critical for developing effective public health interventions in this high-risk occupational group. The primary objective of this study was to comprehensively assess the blood lead levels (BLLs) of battery technicians, and evaluate their current knowledge of lead health hazards, their attitude towards preventive measures, their adherence to safety practices, and their general work habits. This investigation employed a descriptive cross-sectional study design. The study population comprised a total of 150 currently active battery technicians operating within a defined geographical area. Data collection was performed using a structured, pre-tested, self-administered questionnaire. This instrument gathered information on socio-demographics, detailed knowledge of lead's health hazards, specific safety practices utilized, and daily work and personal hygiene habits. The BLLs were concurrently measured for all participants using an appropriate laboratory technique. Statistical analysis, including the Chi-square test, was performed using the Statistical Package for Social Sciences (SPSS), version 20, to test for significant associations, with the significance level set at p≤0.05. Analysis of the data revealed that a substantial proportion of the technicians exhibited elevated BLLs. Key findings indicated that knowledge regarding the appropriate use of a rubber apron, attitude towards the inhalation of lead fumes, and the crucial habit of face washing before eating/smoking were all significantly associated with the measured blood lead level of the battery technicians (p≤0.05). These results underscore that specific behavioral practices directly correlate with the biological burden of lead exposure. The study concludes that there is an urgent need to improve occupational hygiene and health literacy among battery technicians. It is strongly recommended that workplaces ensure the provision and mandatory use of personal protective equipment (PPE), particularly rubber aprons and face masks. Furthermore, intensified health education and regular training on the proper use of PPE, the provision of readily available running water at all workplaces for personal hygiene, and targeted behavioral change communication are essential strategies that will promote consistent personal hygiene habits and, ultimately, reduce the significant occupational lead burden for this vulnerable workforce.},
year = {2025}
}
TY - JOUR T1 - Assessment of Blood Lead Level and Knowledge of Health Hazards, Safety Practices and Work Habits Amongst Battery Technicians in Nigeria AU - Ebenezer Adeiza Ozomata AU - Blossom Adaeze Maduafokwa AU - Opeyemi Giwa AU - Uzoamaka Allena Igwilo AU - Emmanuel Friday Osagiede Y1 - 2025/12/17 PY - 2025 N1 - https://doi.org/10.11648/j.sjph.20251306.13 DO - 10.11648/j.sjph.20251306.13 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 338 EP - 347 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20251306.13 AB - Battery technicians who repair lead-acid batteries are consistently exposed to elemental lead, which poses a significant occupational health risk. This exposure is associated with an elevated risk of developing serious lead related diseases and long-term disability. Understanding the interplay between occupational practices, knowledge of hazards, and actual lead exposure is critical for developing effective public health interventions in this high-risk occupational group. The primary objective of this study was to comprehensively assess the blood lead levels (BLLs) of battery technicians, and evaluate their current knowledge of lead health hazards, their attitude towards preventive measures, their adherence to safety practices, and their general work habits. This investigation employed a descriptive cross-sectional study design. The study population comprised a total of 150 currently active battery technicians operating within a defined geographical area. Data collection was performed using a structured, pre-tested, self-administered questionnaire. This instrument gathered information on socio-demographics, detailed knowledge of lead's health hazards, specific safety practices utilized, and daily work and personal hygiene habits. The BLLs were concurrently measured for all participants using an appropriate laboratory technique. Statistical analysis, including the Chi-square test, was performed using the Statistical Package for Social Sciences (SPSS), version 20, to test for significant associations, with the significance level set at p≤0.05. Analysis of the data revealed that a substantial proportion of the technicians exhibited elevated BLLs. Key findings indicated that knowledge regarding the appropriate use of a rubber apron, attitude towards the inhalation of lead fumes, and the crucial habit of face washing before eating/smoking were all significantly associated with the measured blood lead level of the battery technicians (p≤0.05). These results underscore that specific behavioral practices directly correlate with the biological burden of lead exposure. The study concludes that there is an urgent need to improve occupational hygiene and health literacy among battery technicians. It is strongly recommended that workplaces ensure the provision and mandatory use of personal protective equipment (PPE), particularly rubber aprons and face masks. Furthermore, intensified health education and regular training on the proper use of PPE, the provision of readily available running water at all workplaces for personal hygiene, and targeted behavioral change communication are essential strategies that will promote consistent personal hygiene habits and, ultimately, reduce the significant occupational lead burden for this vulnerable workforce. VL - 13 IS - 6 ER -
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria;Department of Community Medicine, Baze University, Abuja, Nigeria
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria
Department of Community Health, Lagos University Teaching Hospital, Lagos, Nigeria
Department of Community Medicine, Irrua Specialist Teaching Hospital, Irrua, Nigeria;Clinical Science Research, Norwich Medical School, University of East Anglia, Norwich Research Park, United Kingdom